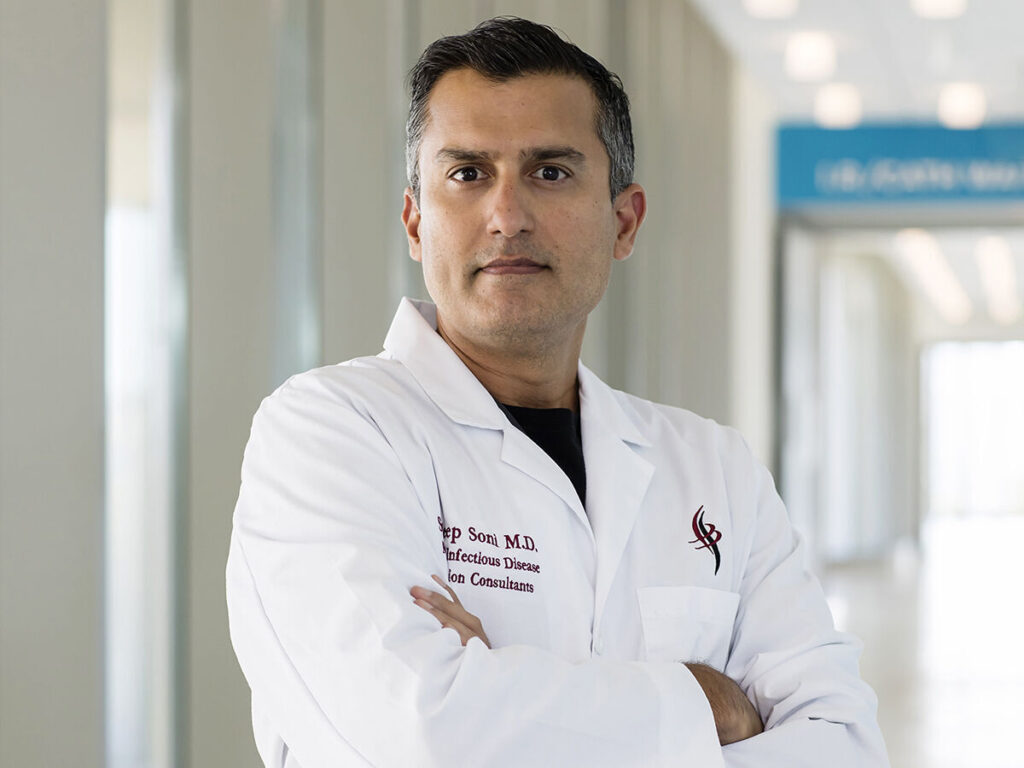
Palomar Health’s infectious disease specialist and medical director, Dr. Sandeep Soni
Jenny Siegwart
Palomar Health admitted its first COVID-19 patient March 13, only two days after the World Health Organization declared the novel coronavirus a global pandemic. However, at both its Poway and Escondido medical centers, preparation had been ongoing for months. Hospital directors produced coronavirus protocols beginning in January, with a strong focus on treating those infected without letting the illness spread to staff or any other patients in the building. They succeeded.
As of press time, Palomar Health had administered 1,075 positive COVID-19 tests since early February, and admitted 389 patients. Yet not a single patient or staff member contracted the virus while on campus during this time.
Leading the effort was infectious disease specialist and medical director Dr. Sandeep Soni, who, like most first responders, felt personally invested in preventing further spread of the coronavirus. “My wife is a critical care specialist at Palomar Health,” he says. Their biggest concern was “making sure we’re not taking everything home to our family.”
Working closely with Dr. Soni was Valerie Martinez, a nurse with three decades’ experience who serves as Palomar’s infection control officer, directing a team of infection preventionists. “We used to be called ‘infection control personnel,’” she clarifies, “but we changed our name across the US to ‘infection prevention,’ because we want to prevent rather than have to go in and try to control it.”
First priority, says Soni, was to increase the hospitals’ number of negative pressure rooms. These rooms are equipped with ventilation systems that keep airborne contagions isolated by siphoning the air flow through filtered exhaust vents that lead outside the building.
Palomar’s two campuses had 27 such rooms between them at the beginning of the year. But its facilities operations department went to work around the clock to convert an additional 57.

Valerie Martinez, infection control officer at Palomar Health.
Jenny Siegwart
In normal times, negative pressure rooms might isolate patients with tuberculosis, or other well-studied infectious diseases. At this point, very little was known about this coronavirus—the CDC wouldn’t advise that its transmission is primarily airborne until May—and the Palomar team was able to disregard public health guidelines calling for only conditional use of negative pressure rooms. Instead, it isolated every patient possible in this way, primarily on its Escondido campus.
They also required facial coverings for everyone entering the hospital from the outset, “before it was a directive from county public health,” notes Martinez. This early action looks prescient now, due not only to the well-publicized risk of asymptomatic spreaders, but also that of presymptomatic carriers. “You can transmit the virus about 48 hours before you start showing symptoms,” she explains.
But Soni and Martinez didn’t have to act on foresight. They based many of their decisions on their experience with another coronavirus. “We had to go through this when SARS was on the map a few years ago,” Soni says. “We put those protocols in place because they were very similar.”
Year-round, Martinez and her team work closely with the county to identify the presence of viruses and bacteria before they spread. But more immediately, they work with the hospitals’ environmental services staff—its cleaning crews.
While the facilities department worked to keep hospital air free of coronavirus, Maria Zaragoza-Magno and 124 other custodial employees were implementing best practices to eradicate it from surfaces. On a daily basis, they don protective gear and thoroughly sanitize the rooms of COVID-19 patients, including those on ventilators. Zaragoza-Magno and her colleagues already possessed the skills needed to safely clean isolation rooms before the pandemic, and now they’ve taken additional measures, like using oxycide, a specialized disinfectant, on high-touch surfaces like faucet handles, light switches, and call buttons.
Dr. Soni points out that the work of environmental services staff carries as much risk of infection as that of doctors and nurses. “They still have to gear up, gown up, put on N95 masks, and go into that room,” he says. “They’ve stepped up.” From top to bottom, the roughly 700 employees at work in the two Palomar hospitals on any given day have all faced the risk of picking up the illness and taking it home to their families. “I don’t think there’s a group of nurses or physicians who have not worked with COVID-19 patients.”
Since the pandemic started, the number of non-coronavirus patients in the hospital has steeply declined, most likely because people are avoiding seeking treatment due to fear of catching the virus. For better or for worse, this has left specialists from other departments available to step in to help with COVID-19’s myriad complications, from thickening blood (thrombosis) to loss of elasticity in the lungs (fibrosis).

Maria Zaragoza-Magno is one of 125 environmental health services workers dedicated to sanitizing the isolation rooms.
Jenny Siegwart
As professional and public understanding of this confounding new illness changed, at times drastically, Soni credits department leaders with helping develop and implement new protocols on the fly. “I think, as a patient, you’re coming into the hospital expecting your physicians to know everything,” he says. “But we were kind of in a no-man’s land.”
A committee of department heads worked together, seven days a week, deliberating over email threads in response to new data and treatment guidance. The pharmacy team fought to secure medications, lab directors sought materials to reduce test result times from days to hours, anesthesiologists implemented plasma transfusion plans, the heads of emergency and critical care kept teams up to date, and the IT staff kept the hospitals’ internal systems updated so providers could successfully order and track shifting courses of treatment.
Soni also lauds the Palomar Health board of directors, who, by May’s end, had spent $4 million to keep the medical centers supplied with materials necessary for both prevention and treatment. In addition to the cost of negative pressure rooms, protective gear, and hard-to-find medications, Palomar Health boosted the number of ventilators on hand from 40 to 160.
Meanwhile, less-invasive treatments have evolved from pursuing unproven long shots (like hydroxychloroquine) to banking on a four-pronged combination supported by the latest research: anticoagulants to prevent thrombosis; plasma infusions from COVID-19 survivors to accelerate immune system response; the corticosteroid dexamethasone to reduce inflammation; and the go-to antiviral drug remdesivir, which has only recently become readily available to all patients who need it.
As September began, 47 Palomar Health patients had died from COVID-19, so the system stood at an 88 percent survival rate, versus 78 percent in San Diego overall. Soni observes that the results have improved since this spring, but he already has his mind set on the upcoming flu season. “How is your body going to react?” he wonders. “That’s the big unknown right now. That’s what keeps me up at night.”
Nevertheless, Martinez stresses that people who need treatment for ailments other than COVID-19 should feel confident and safe in visiting the hospital. “It is safe to come in,” she says.